Disaggregation for Health Equity: Shedding Light on COVID-19’s Impact on the Filipinx Community
Filipinx/a/o (hereafter referred to as Filipinx) Americans are 4% of nurses in the United States but account for 32% of COVID-19 deaths. The aggregation of Asian American COVID-19 data, lumping all Asian subgroups together, obscures the scattered reports that demonstrate a continued surge of Filipinx deaths.
Filipinx Americans make up a significant proportion of nurses, clinical staff, nursing home and home healthcare providers. Many Filipinx Americans care for elderly patients in residential care facilities and critically ill patients in intensive care units. Based on calculations of U.S. census data, one in four of the Filipinx working-age population were essential healthcare workers in 2019.

Nationally, the top country of origin of immigrant healthcare workers who have died from COVID-19 is the Philippines. A Migration Policy Institute study estimates that Filipino immigrants represent the largest share of the United States' 512,000 immigrant registered nurses at 28%.
These trends reflect historical U.S. policies of training and recruiting nurses from the Philippines, once a colony of the United States, to fill U.S. healthcare workforce shortages. As the historian and professor, Catherine Ceniza Choy, noted in her book "Empire of Care: Nursing and Migration in Filipino American History," "U.S. colonialism in the Philippines created an Americanized training hospital system that eventually prepared Filipino women to work as nurses in the U.S. as opposed to the Philippines."
COVID-19 Deaths within the Filipinx Healthcare Workforce
In California, Filipinx Americans make up 3-4% of the population (over 1.6 million people) and a significant proportion of the Asian American population in places like Los Angeles, Riverside, San Diego, San Francisco and Stockton. Filipinx Americans are a substantial portion of the healthcare workforce, making up 20% of the state's nurse population. Following the national trend, over 30% of COVID-19 healthcare worker deaths in California have been Filipinx healthcare workers.


Jollene Levid, a labor organizer and co-founder of AF3IRM, a transnational feminist organization, alongside volunteers, has been tracking the global deaths of healthcare workers of Philippine ancestry on the website KANLUNGAN. The digital memorial has so far chronicled 189 health care workers of Philippine descent who have died from COVID-19 in the U.S. In an interview with NPR, Levid explained that AF3IRM "decided to build Kanlungan.net to both name and honor our fallen healthcare workers of Philippine ancestry." She added that "here in the U.S., we have more than [quadruple] the number of deaths of healthcare workers than the Philippines itself. AF3IRM knew we had to collect this data because no one would do it for us."
In an interview with the Filipino American National Historical Society (FANHS), Levid described KANLUNGAN as a place to "tell our history, the history of Filipino healthcare workers, a place where data could be gathered, and a place where organizers can find stories and testimony to use in campaigns for workplace safety and justice."
For her and so many others, the deaths of healthcare workers are more than just a number. In an interview with CNN, Levid exclaimed, "Why is this happening to our community? There are so many factors, but I would assert that every death was preventable, which is what makes it so much harder."

In Memory of Rosary Castro-Olega
Across the United States, KANLUNGAN and other tribute websites, reports, and articles have documented how Filipinx health care workers are particularly affected. This body of evidence has relied on community advocates, individual case reports, journalists, and obituaries to gauge the impact of COVID-19 on Filipinx health care workers and their families. For Filipinx households, household transmission risks are particularly pronounced as 38% of households are multigenerational and include one or more healthcare workers based on calculations of U.S. census data.
Last May, the children in the Aquino family of Los Angeles tragically grieved the loss of their grandmother, grandfather and their mother, a nurse from the San Fernando Valley, who all passed away due to COVID-19. In July, Roberto Tobias, Jr., a 17-year-old in New York, and his older sister mourned both their parents, who died within a month of each other. Roberto's mother, Loida, was a nurse at Harlem Hospital. Since their passing, Roberto, a high school student, created a GoFundMe page to help support his future college education and desire to one day become a physician. Stories such as these serve as painful reminders of the immense grief this pandemic has brought upon the Filipinx community. Around the country, family members, friends and coworkers of fallen Filipinx healthcare workers are left to mourn.

Decisions Depend on Data
The burden of COVID-19 on the Filipinx American community is hidden in an aggregate Asian category in public-facing data systems. This invisibilization of national and local surveillance data leads to the community being overlooked by policymakers. Vital decisions on resource allocation, outreach, education, economic relief, healthcare and mental health support are being made with aggregate data that mask those disparities.
Multiple studies have shown the unequal burden of diabetes, hypertension, cardiovascular disease and cancer among the Filipinx population. In California, clinically diagnosed type 2 diabetes prevalence is higher among Filipinx adults than Black and Latinx adults, and half of Filipinx individuals with type 2 diabetes remain undiagnosed.
A calculation of restricted California Department of Public Health COVID-19 mortality statistics (as of November 2020) demonstrate that Filipinx health workers have an outsized toll of 6.4% compared to 1.1% for the aggregate Asian category and 0.4% for non-Hispanic Whites.
With the rollout of vaccines and scarcity of vaccine supplies, an evidence-based approach that considers those at the most significant risk of infection should be taken into account. Accepted criteria for equitable allocation of resources by occupation, health risk, work-facility risk and other social and structural determinants of health would include Filipinx Americans as high-priority recipients of vaccines and other support services.
Yet, the extreme case and death tolls indicate systemic discounting — or neglect — of this group. Many Filipinx American home healthcare givers who are undocumented and live in crowded temporary residential apartments will not be included. A class-action lawsuit found a New York nursing home guilty of subjecting 200 Filipinx nurses to unsafe working conditions and violating an anti-trafficking statute (before the pandemic).
Media reports have shown that Filipinx nurses lack access to personal protective equipment (PPE) and work in higher-risk clinical settings. The Philippine government recently introduced a proposal to send nurses to the United Kingdom and Germany to receive COVID-19 vaccines. Filipinx nurses carry a disproportionate burden of care before and during the pandemic due to the high global demand for their expertise.

This systemic mistreatment and potential exploitation of Filipinx nurses can be linked back to a history of U.S. colonialism in the Philippines, which undoubtedly shaped the Philippine educational system and transformed the Philippines into Southeast Asia's biggest exporters of overseas healthcare workers.
A CNN Philippines article featuring Choy elaborated on the linkage:
"The U.S. established an education abroad program in the Philippines called the pensionados program, which worked like a study abroad program. Many Filipino nurses became pensionados; some eventually stayed for employment, while others returned to the Philippines to help set up nursing schools in the country from 1903 to 1940.

"After World War II, the demand for Filipino nurses grew. 'As the United States started to experience nursing shortages after WWII, they started to look abroad to recruit nurses,' Choy says. 'The Philippines became an obvious and important source for nurses in large part because they were American-trained.'
"Choy explains that another wave of nursing shortages started to brew in the 1960s, mainly due to the growing women's movement of that era. As a result, American women had more professional opportunities in all kinds of work. 'Before, they were often relegated as professionals to things that were considered appropriate professions for women, like nursing, education, or social work,' she says."
Today, the need for timely reporting of disaggregated Asian American health outcomes is as urgent as ever. However, most healthcare systems have not publicly reported disaggregated data on the death and infection of Asian Americans. At this stage of the pandemic, accurate reporting of disaggregated Asian American COVID-19 deaths and infections is a matter of improving science and public health.
Accurate reporting of disaggregated COVID-19 health outcomes can help the Filipinx community in the following ways:
- Dispel misconceptions among public health practitioners, healthcare workers, researchers, policymakers and laypeople that COVID-19 is not taking a disproportionate toll on the Filipinx community
- Increase the sense of urgency surrounding COVID-19 vaccination in the Filipinx community, especially among Filipinx Americans with high-risk medical comorbidities (e.g., diabetes, heart disease, obesity and compromised immune systems) not included in the first waves of vaccination
- Strengthen occupational health protections for essential workers, such as frontline healthcare workers and immigrant healthcare workers, who may disproportionately experience discrimination in the workplace
- Optimize allocation of mutual aid (e.g., monetary aid, PPE, and food donations for essential workers)
- Further mobilize the Filipinx community to join health equity initiatives and to build greater solidarity with other communities disproportionately being impacted by COVID-19 (e.g., Black, Latinx, Native American, Native Hawaiian and Pacific Islander communities)
- Recognize the significance of social and structural determinants of health (e.g., income inequity, food insecurity, lack of access to high-quality healthcare, targeted marketing of unhealthy foods, inadequate paid sick leave and hazardous work environments) to the development of chronic-non-communicable diseases that increase the risk of serious COVID-19 infection



Disaggregation is Possible
Before the pandemic, communities advocated for disaggregated health outcomes as there were already concerns that Asian Americans and Native Hawaiians/Pacific Islanders were silently suffering from health inequities. In 2016, California Gov. Jerry Brown signed AB-1726, a law introduced by Assemblymember Rob Bonta. In2022, California will require the state department of public health to break down demographic data for Asian, Native Hawaiian, and Pacific Islander groups. There is mounting concern that this change is not coming soon enough as the U.S. COVID-19 death toll has surpassed 500,000 people.
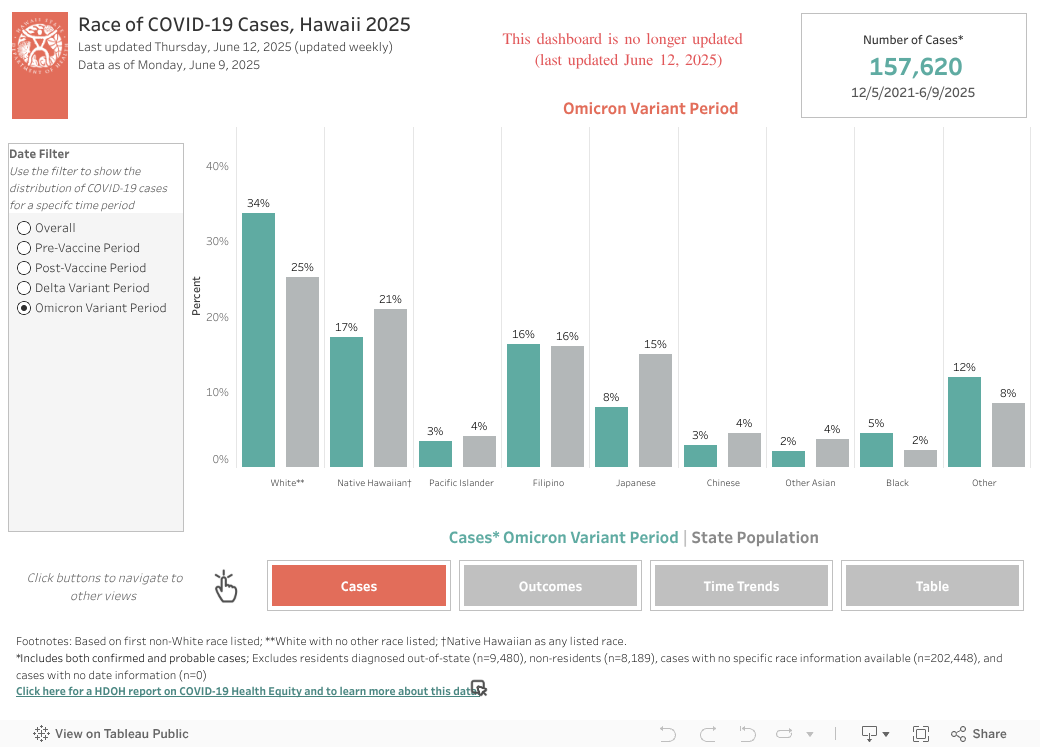
We know that disaggregation is possible and that it reveals critical disparities. In Hawai'i, disaggregated data shows Filipinxs have the second-worst COVID-19 disparities, second only to Pacific Islanders. Filipinxs represent 20% of Hawai'i's COVID-19 cases but only makeup 16% of the population.
Expediting data disaggregation would reveal which communities and, by extension, which individuals may be at disproportionate risk of infection and adverse outcomes from COVID-19. Doing so can help inform individual behavior, targeted interventions, and broader policies to mitigate the pandemic's harm. Perhaps the most salient example of COVID-19 data leading to health policy and resource allocation is the targeted rollout of the COVID-19 vaccines and the prioritization of individuals over 65 and healthcare workers. Early vaccination strategy is consistent with data showing that older individuals and healthcare workers are at greater risk of severe COVID-19 infection and higher infection rates, respectively. Accurate disaggregated data can optimize subsequent vaccine allocation to younger groups at higher risk.
Publicly reporting disaggregated data on social and structural risk factors—including working conditions, sick leave, access to healthcare, access to personal means of transportation, air pollution, food insecurity, multigenerational households, and housing insecurity—is important for responding to COVID-19. Local organizing between Filipinx community leaders, health researchers, clinicians, public health practitioners, sociologists, and policymakers can help bring together epidemiological data, socio-historical context, and real-life stories to make more equitable decisions during the pandemic.
Due to the long history of Filipinx people caring for Americans, which is rooted in U.S. colonialism, it is time that we show Filipinx people that they count, both literally and figuratively. Aggregated data hides the stories of Filipinx Americans' struggle and survival amid the COVID-19 pandemic. Although there are efforts within the Filipinx community to address vaccine hesitancy and provide mutual aid, concrete disaggregated data is necessary for large-scale social and structural change to improve the health and safety of groups disproportionately impacted by this pandemic.