Race, Stress and Poverty: Health Inequities in Spread of COVID-19

Published in partnership with the USC Price Center for Social Innovation in support of the Neighborhood Data for Social Change platform (NDSC): The platform is a free, publicly available online data resource that provides reliable, aggregated data at the city, neighborhood, and census tract level. The mission of the USC Price Center for Social Innovation is to develop ideas and illuminate strategies to improve the quality of life for people in low-income urban communities.
As the number of new COVID-19 cases continues to increase across California and the U.S., Los Angeles has become the state’s hardest-hit county. As of June 24th, the county has 89,490 confirmed cases, and is now leading the nation with the most cases in the U.S.
View COVID-19 cases in Los Angeles County by neighborhood, race/ethnicity, and over time here.
When the outbreak began, county officials were quick to put in place stay-at-home orders to support social distancing, which has been shown to be effective at flattening the curve by lowering transmission rates. However, as Los Angeles County begins moving into different phases of reopening, we are starting to see new spikes in cases, hospitalizations and deaths. Over the weekend of June 6, shortly following the reopening of many businesses for Memorial Day weekend, Los Angeles reported its highest total of new cases (3,000) and COVID-related deaths (81) since April.

Highest-Impacted Communities
The health and economic consequences of the pandemic have not affected all communities across the county equally. At the start of the pandemic, wealthier, Caucasian neighborhoods such as Encino, West Hollywood, Beverly Hills, Santa Monica and Brentwood had initially reported some of the highest infection rates, likely due to the fact that testing was more available in those communities than in lower-income areas. However, those wealthier communities are now seeing much slower growth rates; in contrast, rates in communities of color across South and Central Los Angeles and the Eastside have increased dramatically. These areas now have the highest prevalence of infections in the county, exceeding 600 infections per 100,000 people.

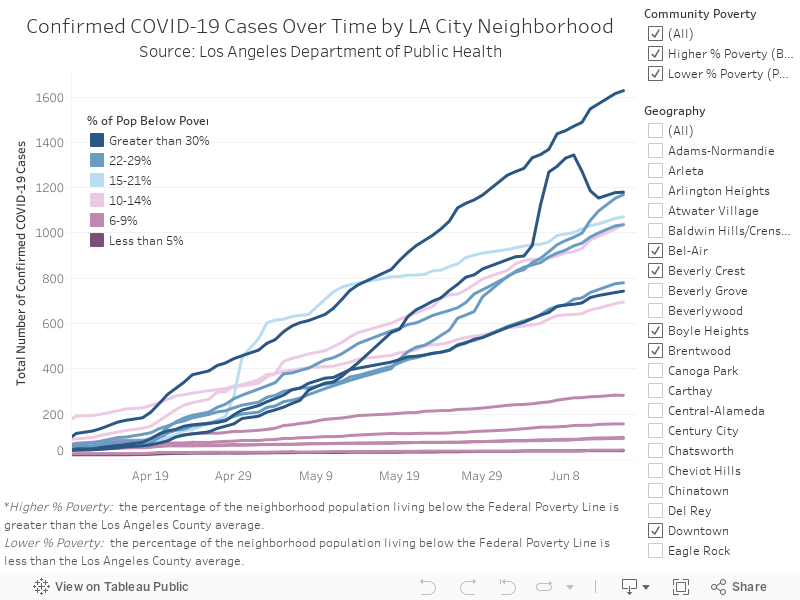
An analysis by RACECOUNTS, an initiative launched by Advancement Project California, USC PERE, PICO California and California CALLS, found that the number of cases in higher-poverty areas (defined as communities where the percentage of residents living under 200% of the Federal Poverty Line is above the median for the county) were 2.7 times higher than the number of cases in lower-poverty areas. Higher-poverty areas also had nearly 4 times as many deaths compared to lower-poverty areas.
Hover over the lines on the chart below to see the total cases, case rate, death rate, poverty levels, and percentage of uninsured population for a specific neighborhood.
When looking at confirmed cases based on race/ethnicity at the city and community levels, the same analysis found that areas with a higher percentage of white residents than the county median had approximately half as many cases as communities with a lower percentage of white residents. These patterns may be the result of higher levels of exposure for low-income and minority populations, who are more likely to work frontline occupations and have more challenges adhering to social distancing guidelines. In Los Angeles County, our analysis found that the Native Hawaiian/Pacific Islander population and the Hispanic/Latino population, have had the highest case rates, while Black and Asian Populations have had the highest death rates.
Racial Disparities in Health Outcomes
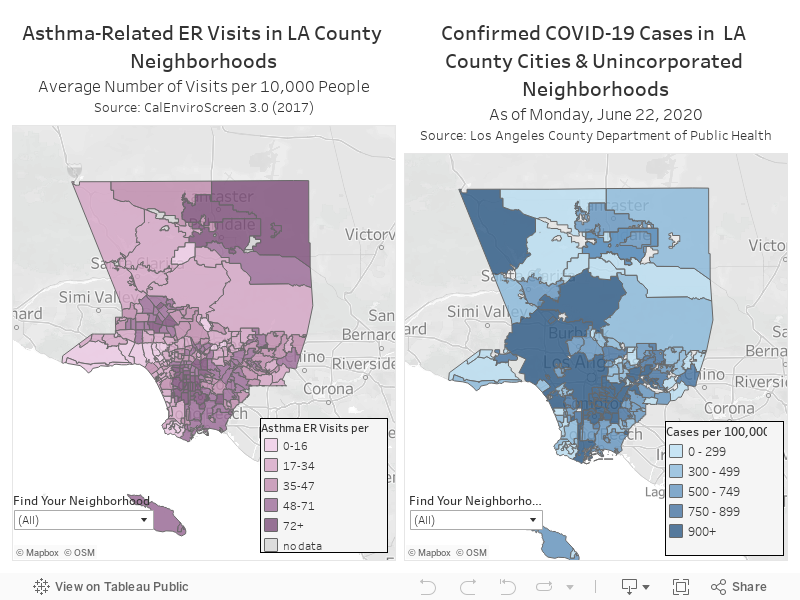
Public health experts have attributed these racial health disparities in COVID-19 cases to a number of compounding factors. A CDC study found the majority of serious COVID-19 cases involve people with underlying health conditions, such as cardiovascular disease, diabetes, and chronic lung disease. Vulnerable populations often have higher rates of serious illnesses, stemming from social determinants of health. For example, many of the neighborhoods in Los Angeles County now experiencing a serious rise in cases are those affected by a disproportionate burden of the county’s environmental pollution, leading to greater health risks that can worsen the outcomes of COVID-19 cases.
The two maps below show the number of Asthma-related ER visits and the number of confirmed COVID-19 cases by neighborhood. Hover over the neighborhoods below to see the specific rates for each.
In addition to environment, public health experts identify the phenomenon of “weathering” as an important factor leading to higher rates of poor health outcomes for communities of color. Termed by Dr. Arline Geronimus, "weathering" refers to the cumulative effects that coping with the stress of discrimination and racism can have on the body. This “wear and tear,” as Dr. Camara Phyllis Jones describes it, may lead to a heightened risk of chronic illnesses that have made the pandemic particularly devastating for these communities.

Lastly, cultural bias that exists within the health care system has led to critical health inequities. The implicit attitudes and behavior of clinicians can cause disparities in access to care, the quality received, and the health outcomes of people of color, even when controlling for income and insurance access. For example, in a national survey conducted in 2017, over 1 in 5 Black Americans reported avoiding needed medical care due to fear of discriminatory treatment from medical professionals. Further, early research by the biotech firm Rubix Life Science, found that Black patients experiencing COVID-19 symptoms during the onset of the pandemic were less likely to get tested or treated than white patients, leading to more severe cases.
Effort to Equalize Access to Health Services
AltaMed Health Services, the nation’s largest independent federally qualified community health center (FQHC), has delivered comprehensive medical services to communities across Southern California since 1969. AltaMed has more than 40 health centers, providing primary care, dental, pediatrics, behavioral health, HIV/AIDS care and prevention services, and senior health programs to nearly 300,000 patients annually. AltaMed predominantly serves Latino and multi-ethnic individuals of all ages, 47% of whom are uninsured. Many of AltaMed's clinicians come from the communities it serves, providing multicultural and bilingual professionals.

AltaMed patients are far more likely than the general public to be uninsured or underinsured and face barriers to accessing health care and health coverage. This is often due to structural barriers and historical factors that have broken trust between low-income minority communities and health systems.
AltaMed serves many of the neighborhoods that are now experiencing some of the highest COVID-19 case rates, such as Westlake, Pico-Union, Downtown Los Angeles and East Hollywood. Recognizing the need for increased testing in some of the most vulnerable communities, AltaMed has become a leader in Southern California’s fight against COVID-19 by providing testing and medical evaluations at five outdoor sites. Additional testing was also made possible by partnering with Los Angeles County.
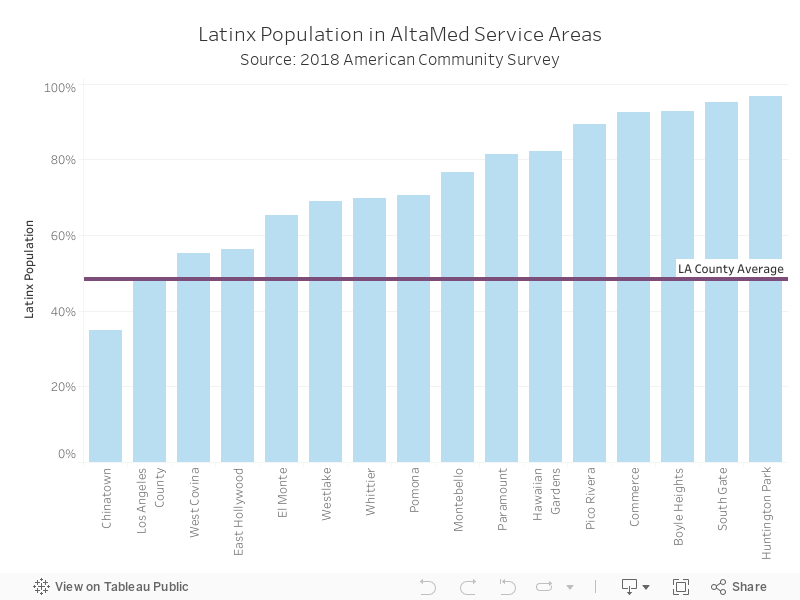
AltaMed's service areas are 74.6% Latinx – compared to the county average of 48.4%. Of those residents, 21.4% are linguistically isolated, meaning they are living in households where no one over the age of 14 speaks only-English or speaks English “very well.” These communities also have higher than average rates of uninsured residents: 15.6% compared to 11.7% countywide. Further, 49.3% of residents live below 200% the Federal Poverty Line and 21% are living in overcrowded housing, meaning there is more than one person per room.
Hover over the bars on the chart below to see the Latinx population, the percentage of households that are limited-English speaking, uninsured population, poverty levels, and percentage of residents living in overcrowded housing for a specific neighborhood.
AltaMed has worked to address the socio-economic barriers that prevent these communities from accessing health care and services. In response to the current pandemic, AltaMed has enhanced telehealth services, with 45% of its visits now occurring through phone and video. This has been paired with free testing, health education services, and a resource guide, as well as the development of best practices for communities of color.
The AltaMed Institute for Health Equity is working to identify and address patients’ social needs that may affect their ability to follow COVID-19 prevention and treatment guidelines. For example, AltaMed is identifying and addressing the needs of patients whose housing status makes adherence to standard COVID-19 guidelines difficult. During intake for all COVID-19-related visits (approximately 1,300 per day as of the beginning of May 2020, including telephonic visits, in-clinic visits, and visits to outdoor evaluation centers ran as testing sites in partnership with Los Angeles County), AltaMed screens all patients about their housing status, including homelessness and overcrowding. Informed by the patients’ housing status, providers then give recommendations from the Centers for Disease Control and Prevention, co-develop plans to maximize social distancing within the unique living situation of the patient, and provide referrals to local housing resources. Printouts with county-specific prevention guidance and resource information are also made available for patients with a focus on resources obtainable through self-referral, such as how to access hygiene stations and safe overnight parking locations established for individuals residing in their vehicles.

AltaMed is also at the forefront of advocacy efforts to ensure that proper resources are deployed to community health centers. AltaMed’s Government Relations Department is working collaboratively with the California Primary Care Association to stop cuts to the 340B Drug Pricing Program, which makes prescription drugs available to low-income populations. AltaMed also co-sponsored a bill to examine how our state can increase the pool of linguistically and culturally competent international medical graduates in California. This is a first step to address the physician shortage crisis faced by diverse communities in California.
AltaMed is also involved in long-term efforts to increase community resources. The FQHC has received nearly $1.3 million in grants to advocate for census completion amongst Los Angeles communities. AltaMed employs 35 Promotoras, who make calls to patients on a daily basis to encourage census participation. Promotoras also visit AltaMed clinics to directly assist patients with census completion. Lastly, AltaMed knows that addressing health disparities requires systems change that can only be accomplished through community empowerment. Consequently, the FQHC will lead voter registration drives and all patient-facing staff will be trained on how to address the importance of voting in local, state and national elections in 2020.
Conclusion
For more than 50 years, AltaMed has been helping to address health inequities in communities of color across Southern California. As the economy begins to reopen, the gaps in our health care system that have been exacerbated under the pandemic will continue to be further aggravated. Given than many impacted neighborhoods across the county will continue to be left at a disadvantage, AltaMed and other organizations working on COVID-specific strategies to help support these communities can play a key role in achieving better health outcomes for Latino and multi-ethnic communities in the region.
Sources
Barboza, Tony, Poston, Ben, Menzes, Ryan (May 28, 2020). Coronavirus ravages poorer L.A. communities while slowing in wealthier ones, data shows. Los Angeles Times.
Center for Disease Control and Prevention (April 17, 2020). Hospitalization Rates and Characteristics of Patients Hospitalized with Laboratory-Confirmed Coronavirus Disease 2019.
Coven, Joshua, Gupta, Arpit (May 15, 2020). Disparities in Mobility Responses to COVID-19. NYU Stern School of Business.
Koran, Mario (June 24, 2020). California sees 69% COVID-19 rise in two days as LA county has most cases in U.S. The Guardian.
Farmer, Blake (April 6, 2020). Long-Standing Racial and Income Disparities Seen Creeping Into COVID-19 Care. Nashville Public Radio.
Geronimus, Arline T., Hicken, Margaret, Keene, Danya, and Bound, John (2006). “Weathering” and Age Patterns in Allostatic Load Scores Among Blacks and Whites in the United States. Am J Public Health.
Harvard T.H. Chan School of Public Health (2020). Air pollution linked with higher COVID-19 death rates.
Robert Wood Johnson Foundation (2020). Discrimination in America: Experience and Views on Affects of Discrimination Across Major Population Groups in the United States.
USC Annenberg (2020). Why do wealthy areas of L.A. have high rates of coronavirus cases?
Villarosa, Linda (April 29, 2020). ‘A Terrible Price’: The Deadly Racial Disparities of Covid-19. The New York Times.